Pulse Amplitude Ratio (PAR)
During brachial artery occlusion peripheral resistance is substantially reduced leading to a pronounced post-occlusive hyperemia in distal arterial segments, depending on bioavailability of nitric oxide due to shear stress. A deficiency of NO, strongly related to endothelial dysfunction, is a hallmark of cardiovascular diseases, predictive of poor clinical outcomes and of other complications [14].
Several testing variants are available in assessing vasomotor function by evaluating perfusion of the digital arteries. Previous studies mainly applied fingertip peripheral arterial tonometry (PAT) to derive pulse volume amplitude changes after reactive hyperemia [15, 16]. This established technique is based on fingertip tonometry with the necessity of rather expensive disposable digital cuffs.
In recent years, novel modalities were developed and introduced applying photo plethysmography in recording of arterial pulse amplitudes [17]. For more than 30 years in clinical and diagnostic use, mainly in internal medicine and angiology, photo plethysmographs, also photo pulse plethysmographs, or PPGs constitute an established technique in evaluating digital perfusion, e.g. for operator independent determination of Ankle Brachial Index (ABI). Among other features the optical PPG signal is able to provide detection of blood volume changes in microvascular beds. The reusable PPG sensor is easily and comfortably clipped to a fingertip, similar to a pulse oximeter.
During brachial artery occlusion peripheral resistance is substantially reduced leading to a pronounced post-occlusive hyperemia in distal arterial segments, depending on bioavailability of nitric oxide due to shear stress. A deficiency of NO, strongly related to endothelial dysfunction, is a hallmark of cardiovascular diseases, predictive of poor clinical outcomes and of other complications [14].
Several testing variants are available in assessing vasomotor function by evaluating perfusion of the digital arteries. Previous studies mainly applied fingertip peripheral arterial tonometry (PAT) to derive pulse volume amplitude changes after reactive hyperemia [15, 16]. This established technique is based on fingertip tonometry with the necessity of rather expensive disposable digital cuffs.
In recent years, novel modalities were developed and introduced applying photo plethysmography in recording of arterial pulse amplitudes [17]. For more than 30 years in clinical and diagnostic use, mainly in internal medicine and angiology, photo plethysmographs, also photo pulse plethysmographs, or PPGs constitute an established technique in evaluating digital perfusion, e.g. for operator independent determination of Ankle Brachial Index (ABI). Among other features the optical PPG signal is able to provide detection of blood volume changes in microvascular beds. The reusable PPG sensor is easily and comfortably clipped to a fingertip, similar to a pulse oximeter.
.

PAR Testing Procedure
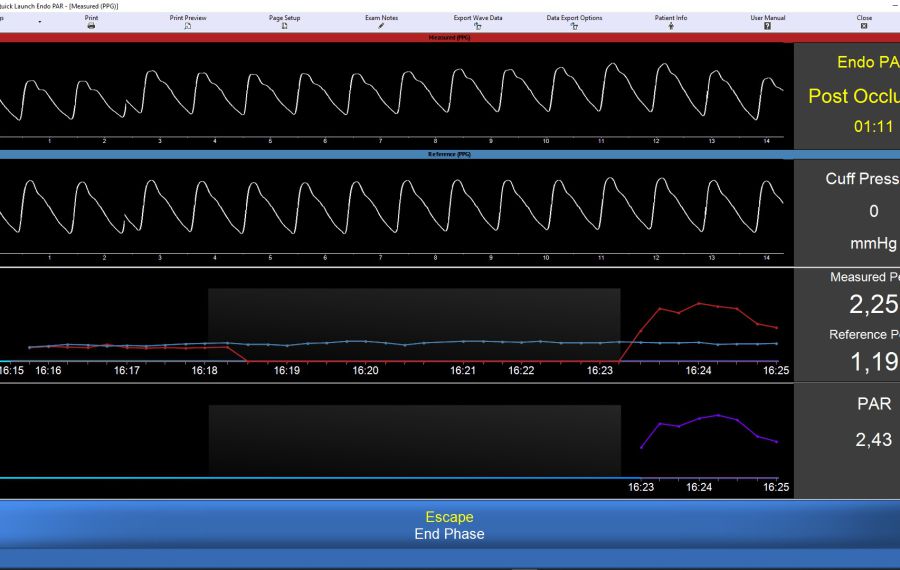
Over the last years, the automated and operator-independent EndoCheck PAR test procedure was developed, now available in the Vicorder® instrument, a proven device in clinical and research applications. EndoCheck PAR profits from many years of experience in FMS testing in the same device. While FSM evaluates the hyperemic response of brachial artery Pulse Wave Velocity, PAR records arterial pulse volume changes in the microvasculature of the fingertip. Reusable photo pulse plethysmograph or PPG sensors are clipped to the two index fingers of the test subject. An inflatable cuff is attached to the upper or forearm on the side where the hyperemic reaction will be tested. The operator is guided through an automated exam procedure, with continuous recording of pulse volume changes derived from the PPG sensor signals. In a pre-recording phase, PPG wave amplitudes are normalized, allowing a real-time evaluation of the test as it proceeds. In addition to the PPG waves, pulse amplitude trend curves from the ipsilateral (test) and contralateral (control) finger are displayed at a slower sweep rate. The cuff is automatically inflated for occlusion of the blood flow to the digital vascular bed on the tested side. During occlusion, complete cessation of blood flow to the ipsilateral finger can be verified by the absence of a PPG signal from the occluded arm, while the PPG wave and the amplitude trend curve of the contralateral side continue to be seen. After release of the cuff pressure, in additotion to pulse amplitude trend curves, the pulse amplitude ratio or PAR is continuously displayed throughout the post-occlusion phase.
During post-occlusive hyperemia, PAR rises as ipsilateral pulse volume amplitudes exceed those of the control side in healthy subjects. A graph is plotted and max. PAR and other test parameters determined. For research purposes test parameters and even pulse amplitude trend curves can be saved in cvs format. In addition, a test report can be printed, stored, or emailed. Durations of pre-occlusiove reference phase,occlusion phase, and post-occlusive phase can be configured by the operator prior to the test exam.
Anticipation of EndoCheck PAR Benefits
In a 2021 publication Cauwenberghs et al. [18] documented their studies of peripheral endothelial dysfunction and its association with subclinical heart abnormalities, the first study of this kind in a general population (n=424). The authors assessed peripheral vasoreactivity by recording digital PPG traces before and during reactive hyperemia, compared the results with signs of cardiac deterioration in echocardiography, and evaluated cardiovascular risk, e.g. by looking at left ventricular hypertrophy (LVH) and remodeling as well as diastolic dysfunction.
The authors conclude:
“Microvascular endothelial function may be an important phenotype for risk stratification, diagnosis and prognosis of heart failure with preserved ejection fraction (HFpEF). Peripheral endothelial dysfunction may represent a valid surrogate of coronary microvascular dysfunction for detection of individuals at risk for cardiac deterioration.
In line, the digital vasoreactive response identified patients with coronary endothelial dysfunction with high sensitivity and specificity.”
Although the device used in this publication for evaluating digital reactive hyperemia was a commercially not available instrument, the authors have also been using Vicorder® for determination of microvascular endothelial function through PAR.
Vicorder EndoCheck PAR is a non-invasive exam evaluating digital reactive hyperemia with photo pulse plethysmography (PPG), using the same modality as above. The operator-independent test is simple to apply, safe and convenient for patient. The automated test progression can be viewed and verified by the operator at all times throughout the exam. Results are immediately available at the end of the test and do not require post-processing. All data, including PPG amplitude traces, can be exported and/or results printed. Sensors are reusable, so there is not recurrent cost associated with EndoCheck PAR.
Its release pending, EndoCheck PAR will be available soon.
For more info on VICORDER® EndoCheck click here.